Certified Professional Coder (CPC) Exam Questions and Answers
(What is the medical term for the study of the kidney?)
According to the Application of Cast and Strapping CPT® guidelines, what is reported when an orthopedic provider performs initial fracture care treatment for a closed scaphoid fracture of the wrist, applies a short arm cast, and the patient will be returning for subsequent fracture care?
A 47-year-old female presents to the operating room for a partial corpectomy on one upper thoracic vertebral body, T3. Two surgeons are performing the surgery. One surgeon performs the transthoracic approach and excises the damaged portion of the vertebral body. The second surgeon inserts a bone graft into the vertebral gap, closing the gap, and inserts a metal plate. Both surgeons work together, each as a primary surgeon.
How does each surgeon report their portion of the surgery?
(Full Case:Chief complaint:Syncope.HPI:68-year-old male arrives to ED inrespiratory distressafter sudden syncope/collapse while shopping; unresponsive; EMS: weak pulse, labored respirations, unresponsive. History:CABG 5 years ago, no chest pain since.ROS:unobtainable (unconscious).Allergies:none.Meds:Coumadin.PMH:HTN.Social:lives with wife.Exam/Vitals:BP 82/62, pulse 79, RR 12 shallow, O2 sat 90% on high flow O2; monitor shows right bundle branch block. Neuro: initially eyes closed, opens to questions, responds to some questions, later unresponsive. HEENT pupils sluggish equal; unable EOM/fundus. Neck supple, no JVD/bruits. Lungs mild rhonchi. Heart regular without murmurs. Abdomen benign. Extremities symmetric, no edema/cyanosis. Skin no rash. Neuro no focal deficits.Hospital course:IV x2; NS 1000 cc bolus with little response; dopamine drip 10 → 20 mcg/kg/min; O2 sat drops, respirations slow; becomes unresponsive; progresses tocardiac arrest; CPR; multiple adrenaline/atropine; defibrillation; ABG pH 7.1 etc; bicarbonate x2; no effect; pronounced dead 13:32.Critical care time:77 minutes continuous.Diagnosis:Cardiorespiratory arrest.Question:What is the E/M coding reported for this encounter?)
A patient presents with fever, cough, SOB, and a recent history of COVID-19. A PCR test was positive for COVID-19. The provider documents a final diagnosis of “pneumonia with history of COVID-19.”
What ICD-10-CM coding is reported?
A patient is diagnosed with sepsis and associated acute respiratory failure.
What ICD-10-CM code selection is reported?
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
Which CPT® and ICD-10-CM codes are reported for this procedure?
Which place of service code is submitted on the claim for a service that is performed in a skilled nursing facility?
A Medicare patient that is on dialysis for ESRD is seen by the nurse for a Hep B vaccination. This patient is given a dialysis patient dosage as part of a three-dose schedule. The nurse administers the Hep B vaccine in the right deltoid. The physician reviews the chart and signs off on the nurse ' s note.
What procedure and diagnosis codes are reported for the scheduled vaccine injection for this Medicare patient?
A patient with malignant lymphoma is administered the antineoplastic drug Rituximab 800 mg and then 100 mg of Benadryl.
Which HCPCS Level II codes are reported for both drugs administered intravenously?
Which government office is responsible for overseeing and investigating cases of healthcare fraud and abuse?
(What ICD-10-CM coding is reported forType 1 diabeteswithdiabetic chronic kidney disease?)
A cardiologist performs and interprets a 12-lead ECG in the office.
What CPT® coding is reported?
Patient has esotropia of the right eye and presents to operating suite for strabismus surgery. The physician resects the medial rectus horizontal and lateral rectus muscles of the eye and secures them with adjustable sutures. Extensive scar tissue is noted, due to a previous surgery involving an extraocular muscle. Extraocular muscle is isolated, and the muscle is freed from surrounding scar tissues.
What CPT® codes are reported for this surgery?
Refer to the supplemental information when answering this question:
View MR 138093
What E/M coding is reported?
Which punctuation is used in the ICD-10-CM Alphabetic Index to identify manifestation codes?
A patient with empyema requires a Schede thoracoplasty.
What CPT® code is reported for this procedure?
A physician sees a patient for the first observation visit, spends 85 minutes, with moderate MDM.
What CPT® code is reported?
A couple presents to the freestanding fertility clinic to start in vitro fertilization. Under radiologic guidance, an aspiration needle is inserted (by aid of a superimposed guiding-line) puncturing the ovary and preovulatory follicle and withdrawing fluid from the follicle containing the egg.
What is the correct CPT® code for this procedure?
Refer to the supplemental information when answering this question:
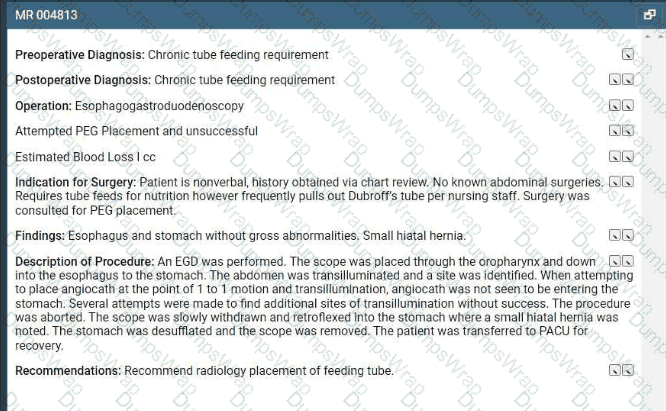
View MR 004813
What CPT® and ICD-10-CM codes are reported?
A 45-year-old male, with no prior history of heart disease, has been diagnosed having atherosclerotic heart disease with unstable angina. He is in the cardiologist ' s office for a cardiac MRI test
to determine the morphology and function of his heart under stress. First images obtained are without contrast and then contrast is administered for the next set of images. Then the physician
injects medicine to increase the heart rate and checks the coronary arteries for narrowing or blockage. Physician interprets the test and the results and images are in the medical record.
What radiology CPT® and ICD-10-CM codes are reported?
Two weeks after removal of a 4 cm subcutaneous lipoma, the patient presents with extensive internal wound dehiscence requiring multi-layer closure in the OR.
What CPT® coding is reported by the surgeon?
A patient suffers a ruptured infrarenal abdominal aortic aneurysm requiring emergent endovascular repair. An aorto-aortic tube endograft is positioned in the aorta and a balloon dilation is performed at the proximal and distal seal zones of the endograft. The balloon angioplasty is performed for endoleak treatment.
What CPT® code does the vascular surgeon use to report the procedure?
(A male patient passes out while jogging in the park. Upon examination at the hospital, he is found to have a wide complex tachycardia and undergoes anelectrophysiologic study and radiofrequency ablation. For this procedure he is placed undergeneral anesthesia. What is the anesthesia coding for this otherwise healthy 35-year-old?)
The spleen is in what organ system?
A 42-year-old male is diagnosed with a left renal mass. Patient is placed under general anesthesia and in prone position. A periumbilical incision is made and a trocar inserted. A laparoscope is inserted and advanced to the operative site. The left kidney is removed, along with part of the left ureter. What CPT® code is reported for this procedure?
The CPT® code book provides full descriptions of medical procedures, although some descriptions require the use of a semicolon (;) to distinguish among closely related procedures.
What is the full description of CPT® code 69644?
A patient undergoes right thyroid lobectomy for malignancy and removal of a suspicious parathyroid gland.
What CPT® codes are reported?
A 30-year-old patient with a scalp defect is having plastic surgery to insert tissue expanders. The provider inserts the implants, closes the skin, and increases the volume of the expanders by injecting saline solution. Tissue is expanded until a satisfactory aesthetic outcome is obtained to repair the scalp defect.
What CPT® code is reported?
Refer to the supplemental information when answering this question:
View MR 623654
What CPTO coding is reported for this case?
An MRI guided cisternal puncture with diagnostic contrast injection is performed at the C2 level for cervical discography, with imaging supervision and interpretation.
What CPT® coding is reported?
(A patient is in her otolaryngologist’s office to receive therapeutic treatment forasthmatic bronchitis with status asthmaticus. A subcutaneous injection ofomalizumab (150 mg)is given in her left upper arm. What is the CPT® and ICD-10-CM coding?)
A 10-year-old had a cochlear implant in his left ear few weeks ago. Today he sees the audiologist to initialize and program the implant.
What CPT® code is reported?
A 65-year-old man had a right axillary block by the anesthesiologist. When the arm was totally numb, the arm was prepped and draped, and the surgeon performed tendon repairs of the right first, second, and third fingers. The anesthesiologist monitored the patient throughout the case.
What anesthesia code is reported?
A patient with suspected gynecologic malignancy undergoes laparoscopic staging including bilateral pelvic lymphadenectomy, periaortic lymph node sampling, peritoneal washings, peritoneal and diaphragmatic biopsies, and omentectomy.
What CPT® coding is reported?
A flexible sigmoidoscopy is performed with ablation of two sigmoid colon polyps.
What CPT® and ICD-10-CM codes are reported?
A surgeon performs midface LeFort I reconstruction on a patient’s facial bones to correct a congenital deformity. The reconstruction is performed in two pieces in moving the upper jawbone forward and repositioning the teeth of the maxilla of the mid face.
What CPT® code is reported?
What is the HCPCS Level II code for a standard wheelchair?
Dr. Meredith sees Mr. Hollis (new patient) for the first time In the Community Rest Home. She documents a visit with medical decision making of moderate complexity. She spends 20 minutes of additional time discussing physical therapy and going over medications. Dr. Meredith spends a total of 90 minutes on that patient that day.
What CPT® coding does Dr. Meredith report?
(A trauma patient needs the following imaging:2 views nasal bones,3 views chest,2 views left forearm,2 views tibia/fibula. To exclude stroke, aCTA head with contrastis also ordered. What CPT® coding is reported?)
Refer to the supplemental information when answering this question:
View MR 005271
What CPT® coding is reported?
(A patient is diagnosed with agangrenous ulceron theright thighwith thefat layer exposedand is currently being treated. What ICD-10-CM coding is reported?)
Which statement is FALSE in reporting a personal history ICD-10-CM code?
View MR 004397
MR 004397
Operative Report
Preoperative Diagnosis: Calculi of the gallbladder
Postoperative Diagnosis: Calculi of the gallbladder, chronic cholecystitis
Procedure: Cholecystectomy
Indications: The patient is a 50-year-old woman who has a history of RUQ pain, which ultrasound revealed to be multiple gallstones. She presents for removal of her gallbladder.
Procedure: The patient was brought to the OR and prepped and draped in a normal sterile fashion. After adequate general endotracheal anesthesia was obtained, a trocar was placed and C02 was insufflated into the abdomen until an adequate pneumoperitoneum was achieved. A laparoscope was placed at the umbilicus and the gallbladder and liver bed were visualized. The gallbladder was enlarged and thickened, and there was evidence of chronic inflammatory changes. Two additional ports were placed and graspers were used to free the gallbladder from the liver bed with a combination of sharp dissection and electrocautery. Cystic artery and duct are clipped. Dye is injected in the gallbladder. Cholangiography revealed no intraluminal defect or obstruction. Gallbladder is dissected from the liver bed. The scope and trocars are removed.
What CPT® coding is reported for this case?
Patient has cervical spondylosis with myelopathy. The surgeon performed a bilateral posterior laminectomy with facetectomies at each level and foraminotomies performed between interspaces C5-C6 and C6-C7. Bilateral decompression of the nerve roots is achieved.
What CPT® coding is reported?
Which statement is NOT true regarding the ICD-10-CM coding guidelines for burns?
A cystic lesion on the chest is excised with margins totaling 2.5 cm. Simple closure performed.
What CPT® coding is reported?
A patient presents with keratosis lesions on her left cheek, above the left eyebrow, and on the chin area. The dermatologist treats those areas by lightly sanding the surface of a total of 5 lesions.
What CPT® coding is reported?
Which entity offers compliance program guidance to form the basis of a voluntary compliance program for a provider practice?
(What modifier is appended to indicate that during thepostoperative period, a procedure is performed that wasplanned,more extensivethan the original procedure, or done fortherapeutic reasons?)
A CRNA independently administers MAC anesthesia for ICD replacement.
What CPT® and ICD-10-CM codes are reported?
A patient arrives at the clinic experiencing pain due to a chest injury caused by blunt force. The provider takes X-ray imaging with 6 views of the chest.
What CPT® coding is reported?
(A 1-year-old patient was born with twosupernumerary digits, one extending from the right pinky and one extending from the left pinky. The digit from his left pinky is larger and includes themetacarpal bone with a jointand is amputated. The one on the right is anubbinand containsno bony structure. The hand surgeon removes the extra digit containingsoft tissueby a simple excision. What is the CPT® coding for the procedures performed?)
A patient underwent a colonoscopy, where the gastroenterologist biopsied two polyps from the colon. Each polyp was sent to pathology as separately identified specimens. The gastroenterologist was requesting a pathology consult while the patient was still on the table. Tissue blocks and frozen sections were then prepared and examined as follows:
Specimen 1: First Tissue Block—Three Frozen Sections Second Tissue Block—One Frozen Section Specimen 2: First Tissue Block—Two Frozen Sections Second Tissue Block—One Frozen Section
What CPT® coding is reported?
(What is the ICD-10-CM code for amedial meniscus tearof theleft kneedue to arecent football injury?)
A 60-year-old male suffering from degenerative disc disease at the L3-L4 and L5-S1 levels was placed under general anesthesia. Using an anterior approach, the L3-L4 disc space was exposed. Using blunt dissection, the disc space was cleaned. The disc space was then sized and trialed. Excellent placement and insertion of the artificial disc at L3-L4 was noted. The area was inspected and there was no compression of any nerve roots. Same procedure was performed on L5-S1 level. Peritoneum was then allowed to return to normal anatomic position and entire area was copiously irrigated. The wound was closed in a layered fashion. The patient tolerated the discectomy and arthroplasty well and was returned to recovery in good condition. What CPT® coding is reported for this procedure?
The mediastinum is:
A patient returns for embryo transfer. The lab thaws cryopreserved embryos and cultures them for two additional days.
What CPT® coding is reported?
Patient has a 5 cm tumor in the left lower quadrant abdominal wall. A horizontal skin incision is made directly over the tumor in the patient ' s left lower quadrant and dissection was carried
down through the dermis and subcutaneous tissue. The tumor is located and completely excised using electrocautery. The specimen is sent immediately to pathology to rule out cancer. What
CPT® and ICD-10-CM codes are reported?
View MR 099407
MR 099407
Emergency Department Visit
Chief Complaint: VOMITING.
This started just prior to arrival and is still present. He has had nausea and vomiting. No diarrhea, black stools, bloody stools or abdominal pain. Pt is diabetic and has been having elevated blood sugars (320 mg/dL).
REVIEW OF SYSTEMS: Unobtainable due to patient ' s altered mental status.
PAST HISTORY: Poorly controlled diabetes mellitus, with history of poor compliance.
Medications: See Nurses Notes.
Allergies: PCN.
SOCIAL HISTORY: Nonsmoker. No alcohol use or drug use.
ADDITIONAL NOTES: The nursing notes have been reviewed.
PHYSICAL EXAM
Appearance: Lethargic. Patient in mild distress.
Vital Signs: Have been reviewed-tachycardic.
Eyes: Pupils equal, round and reactive to light.
ENT: Dry mucous membranes present.
Neck: Normal inspection. Neck supple.
CVS: Tachycardia. Heart sounds normal. Pulses normal.
E D. Course: Insulin IV drip per protocol, at 10 units/hr.
Zofran 8 mg 01:33 Jul 13 2008 IVP.
Phenergan 25 mg IVP. 07:52.Discussed case with physician. Dr. X. Reviewed test results. Agreed upon treatment plan. Physician will see patient in hospital.
Total critical care time: 45 min.
Disposition: Admitted to Intensive Care Unit. Condition: stable.
Admit decision based on need for monitoring and IV hydration and medications.
CLINICAL IMPRESSION: Vomiting, diabetic ketoacidosis, probable diabetes insipidus.
What E/M code is reported for this encounter?
A 62-year-old with ventricular fibrillation comes to the outpatient surgery department for the replacement of a pacing cardioverter-defibrillator. The procedure is performed under MAC
anesthesia. The Certified Registered Nurse Anesthetist (CRNA), is working independently without medical direction.
What CPT® and ICD-10-CM codes are reported for the CRNA?
A physician performs excisional debridement on multiple wounds:
Lower back: 12 cm, involving fascia
Left shoulder: 8 cm, involving subcutaneous tissue
Left lower leg: 16 cm, involving subcutaneous tissue
What CPT® codes are reported?
What does the suffix -graph mean?
(Full Case:Pre/Post-op diagnosis:Grade 1 endometrial cancer.Procedure:Radical hysterectomy and pelvic lymph node sampling.Anesthesia:General.EBL:400 mL.Complications:None.Specimens:pelvic washings; uterus; tubes; ovaries; pelvic lymph nodes.Fluids:2 L crystalloid.Operative details:frog-leg position; perineum prepped sterile; Foley placed; midline vertical incision umbilicus to symphysis; exploration shows normal upper abdomen and bowel; no paraaortic adenopathy; pelvis/perineum normal; washings collected; round ligaments transected; retroperitoneal spaces opened; ureters visualized; ovarian vessels isolated/ligated; bladder flap taken down; uterine arteries, uterosacral and cardinal ligaments clamped/ligated; uterus removed; vagina closed; lymph node sampling left then right with removal of lymphatic tissue from external/internal iliac bifurcation to circumflex iliac vein and down to obturator nerve; tumor ~40% endometrial surface with < 50% myometrial invasion; closure in layers; patient tolerated well.Question:What CPT® codes are reported?)
What is the muscular ring around a lumen that contracts to control flow through that lumen called?
A patient is diagnosed with a healing pressure ulcer on her left heel that is currently being treated.
What ICD-10-CM coding is reported?
A physician excises a 3.5 cm malignant lesion including margins from the back. Then a destruction of a 2.0 cm benign lesion on the right cheek of the face with cryosurgery.
What CPT@ and ICD-10-CM is reported?
View MR 099405
MR 099405
CC: Shortness of breath
HPI: 16-year-old female comes into the ED for shortness of breath for the last two days. She is an asthmatic.
Current medications being used to treat symptoms is Advair, which is not working and breathing is getting worse. Does not feel that Advair has been helping. Patient tried Albuterol for persistent coughing, is not helping. Coughing 10-15 minutes at a time. Patient has used the Albuterol 3x in the last 16 hrs. ED physician admits her to observation status.
ROS: No fever, no headache. No purulent discharge from the eyes. No earache. No nasal discharge or sore throat. No swollen glands in the neck. No palpitations. Dyspnea and cough. Some chest pain. No nausea or vomiting. No abdominal pain, diarrhea, or constipation.
PMH: Asthma
SH: Lives with both parents.
FH: Family hx of asthma, paternal side
ALLERGIES: PCN-200 CAPS. Allergies have been reviewed with child’s family and no changes reported.
PE: General appearance: normal, alert. Talks in sentences. Pink lips and cheeks. Oriented. Well developed. Well nourished. Well hydrated.
Eyes: normal. External eye: no hyperemia of the conjunctiva. No discharge from the conjunctiva
Ears: general/bilateral. TM: normal. Nose: rhinorrhea. Pharynx/Oropharynx: normal. Neck: normal.
Lymph nodes: normal.
Lungs: before Albuterol neb, mode air entry b/l. No rales, rhonchi or wheezes. After Albuterol neb. improvement of air entry b/l. Respiratory movements were normal. No intercostals inspiratory retraction was observed.
Cardiovascular system: normal. Heart rate and rhythm normal. Heart sounds normal. No murmurs were heard.
GI: abdomen normal with no tenderness or masses. Normal bowel sounds. No hepatosplenomegaly
Skin: normal warm and dry. Pink well perfused
Musculoskeletal system patient indicates lower to mid back pain when she lies down on her back and when she rolls over. No CVA tenderness.
Assessment: Asthma, acute exacerbation
Plan: Will keep her in observation overnight. Will administer oral steroids and breathing treatment. CXR ordered and to be taken in the morning.
What E/M code is reported?
(From the left femoral artery, the catheter was advanced into the abdominal aorta, andaortographywas performed to view the location of the left inferior phrenic artery. Next the catheter was advanced into theleft inferior phrenicand into theleft superior suprarenal (adrenal) arteryand angiography was performed. The angiography showed no blockage of the left adrenal artery. What CPT® codes are reported?)
(Which punctuation is used in the ICD-10-CM Tabular List to denotesynonyms, alternative wording, or explanatory phrases?)
A patient undergoes MRI-guided needle liver biopsy with two core samples taken.
What CPT® codes are reported?
View MR 007400
MR 007400
Radiology Report
Patient: J. Lowe Date of Service: 06/10/XX
Age: 45
MR#: 4589799
Account #: 3216770
Location: ABC Imaging Center
Study: Mammogram bilateral screening, all views, producing direct digital image
Reason: Screen
Bilateral digital mammography with computer-aided detection (CAD)
No previous mammograms are available for comparison.
Clinical history: The patient has a positive family history (mother and sister) of breast cancer.
Mammogram was read with the assistance of GE iCAD (computerized diagnostic) system.
Findings: No dominant speculated mass or suspicious area of clustered pleomorphic microcalcifications is apparent Skin and nipples are seen to be normal. The axilla are unremarkable.
What CPT® coding is reported for this case?
Which is a malignant neoplasm originating in the skin?
(A three-year-old patient returns forstage 2treatment for double right outlet syndrome. The surgeon removes apulmonary artery bandand performstransposition repair of the great vesselsvia aortic pulmonary reconstruction. Central cannulae are inserted forECMO bypass, chemical cardioplegia is initiated, and a physician assistant monitors vitals and oxygenation until heart function resumes. What CPT® codes are reported for the surgery today?)
An anesthesiologist medically directs two cases during EGD and colonoscopy in a PS III patient with severe bleeding risk.
What CPT® codes are reported?
A patient has suspicious lesions on his feet. Biopsies confirm squamous cell carcinoma. The patient elects to destroy a 0.6 cm lesion on the right dorsal foot and a 2.0 cm lesion on the left dorsal foot using cryosurgery.
What CPT® coding is reported?
Refer to the supplemental information when answering this question:
View MR 000281
What anesthesia and diagnosis codes are reported for this case?
A patient presents to the emergency room with a nosebleed that is controlled by limited anterior nasal packing.
What CPT® code is reported?
A patient who is 37 weeks ' gestation is admitted to labor and delivery for a cesarean delivery. An external cephalic version was performed successfully several days ago and she now presents in labor, fully dilated, and the fetus has returned to a footling presentation.
What anesthesia code is reported?
An incision is made in the scalp, a craniectomy is performed to access the area where electrodes are present. The electrodes are removed. The surgical wound is closed.
What procedure code is reported?
Adenoids, tonsils, appendix, and spleen belong to which organ system?
Patient is admitted in observation care on 12/2/20XX in the morning for acute asthma exacerbation. The ED physician requires the patient to stay overnight. Next day, 12/3/20XX the patient is
discharged from observation care in the afternoon. Patient ' s total stay in observation was 16 hours.
What E/M categories and code ranges are appropriate to report?
A patient comes in complaining of pain in the lower left back, which is accompanied by a numbing sensation that extends into the leg. Attempts to alleviate the pain with home treatments have been unsuccessful. The provider orders an MRI of the lumbar spine initially without, and then with, contrast material. The images are interpreted by the physician, the final diagnosis is left-sided low back pain with sciatica.
What CPT® and ICD-10-CM codes are reported?
A patient with three thyroid nodules is seen for an FNA biopsy. Using ultrasonic guidance, the provider inserts a 25-gauge needle into each nodule. Nodular tissue is aspirated and sent to pathology.
What CPT® coding reported?
Patient had polyps removed on a previous colonoscopy. The patient returns three months later for a follow-up examination for another colonoscopy. No new polyps are seen.
What diagnosis coding is reported for the second colonoscopy?
A 13-year-old established patient is seen for an annual preventive exam. Last visit was two years ago.
What CPT® code is reported?
A patient is diagnosed with sepsis due to enterococcus. What ICD-10-CM code is reported?
(A patient with abnormal growth had asuppression studythat includedfive glucose testsandfive human growth hormone tests. What CPT® coding is reported?)
(A patient visits her provider’s office because she is experiencing persistent headaches. Her provider sends her to a radiology facility to do aCT scan of the brain without contrast. The images are sent to the provider, and the providerreads and interpretsthe scan. What CPT® coding of the radiology service is reported by the provider?)
(A patient has nausea with several episodes of emesis and severe stomach pain due to dehydration. Normal saline is infused in the same bag with2 mg ondansetron. Then15 mg ketorolac tromethamineis given for stomach pain. What J codes are reported for these services?)
A patient had surgery a year ago to repair two extensor tendons in his wrist. He is in surgery for a secondary repair for the same two tendons with free graft. What CPT® coding is reported?
Regarding the CPT® Surgery Guidelines for a surgical code designated as a " Separate Procedure " , which statement is FALSE?
Which CPT® code can have modifier 26 appended to it?
What does the prefix “sub-” signify in medical terminology?
(A 52-year-old woman has vulvar intraepithelial neoplasia (VIN II). The surgeon performs avulvectomyremovingless than 80%of the vulva, including affected skin and deep subcutaneous tissue. What CPT® and ICD-10-CM codes are reported?)
(A patient is in her dermatologist’s office for treatment of recurring psoriatic plaques on the upper back and neck resistant to topical therapy. The dermatologist performsExcimer laser therapyon the upper back (300 sq cm) and neck (100 sq cm), total surface area400 sq cm. What CPT® codes are reported?)
A Medicare patient is scheduled for a screening colonoscopy.
What code is reported for Medicare?
Mr. Woolridge has had a suspicious lesion on his left shoulder for approximately eight weeks that is not healing. On the dermatologist ' s exam of left shoulder blade, there is excoriation and scabbing and the lesion not healing. Patient agrees and wishes to proceed with a punch biopsy of the lesion. A punch biopsy is taken of the lesion and sent to pathology. A simple repair is performed at the biopsy site.
What CPT® and ICD-10-CM codes are reported?
In rhinoplasty:
Mrs. Wilder presents with right and left leg swelling. Venous thrombosis imaging of each leg is done and shows deep venous embolism and thrombosis in each leg.
What CPT® and ICD-10-CM codes are reported?
A 52-year-old woman has been experiencing discomfort and itching In the vulvar area for several months. She has a history of abnormal Pap smears and a recent biopsy revealed vulvar intraepithelial neoplasia (VIN III). Decision has been made to perform a vulvectomy.
Procedure: Under general anesthesia, the surgeon made an incision in the vulvar area and removed the vulva (more than 80%), including the affected skin and deep subcutaneous tissue.
What CPT® and ICD-10-CM codes are reported?
A 45-year-old patient comes In with chronic sinusitis that has not responded to medication. The physician decides to use a sinus stent implant to help alleviate the patients symptoms.
The physician inserts the implant into the ethmoid sinus using a delivery system. This implant is designed to keep the surgical opening clear, prop open the sinus, and gradually release a corticosteroid with anti-inflammatory properties directly to the sinus lining. The implant is not permanent and will dissolve over time.
What HCPCS Level II code is reported?
An otolaryngologist removes a 3 cm deep facial tumor within muscle.
What CPT® code is reported?
A 52-year-old male patient with known AIDS saw his orthopedic physician today for severe pain in the right knee. The physician documents that his knee pain is due to a flare up of posttraumatic osteoarthritis and he gives him a cortisone injection in the right knee joint. The osteoarthritis is not related to AIDS.
What ICD-10-CM codes are reported for this encounter?
(Full Case:Preoperative diagnosis:Low back pain; possible spinal stenosis L3–4.Postoperative diagnosis:No evidence of discogenic pathology or spinal stenosis at L3–4; normal discography L3–4.Procedure:Awake discography and injection, L3–4.Anesthesia:IV narcotic with reversal and local; propofol given transiently, then patient alert/responsive for pain response during injection.Technique:Patient to OR; right decubitus; sterile prep/drape; C-arm used to mark entry; local ethyl chloride + 1% Xylocaine; docking needle placed posterolateral at L3–4 under AP/lateral; inner needle advanced to disc nucleus center; contrast injected while monitoring patient response; normal bilocular pattern; 1.5 cc volume; no pain with pressurization.Documentation:No videotape; plain films available; post-discography CT planned/reviewed for other causes.Question:What CPT® and ICD-10-CM coding is reported?)
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
What CPT® codes are reported?
The patient, who is at 32 weeks pregnant, has been hospitalized due to an infection of COVID-19.
What ICD-10-CM codes are reported?
(A 62-year-old with insulin-dependent diabetes mellitus has sudden hearing loss. The otolaryngologist administered atranstympanic injection of a steroidfor the sudden hearing loss ineach ear. How is this reported?)
Refer to the supplemental information when answering this question:
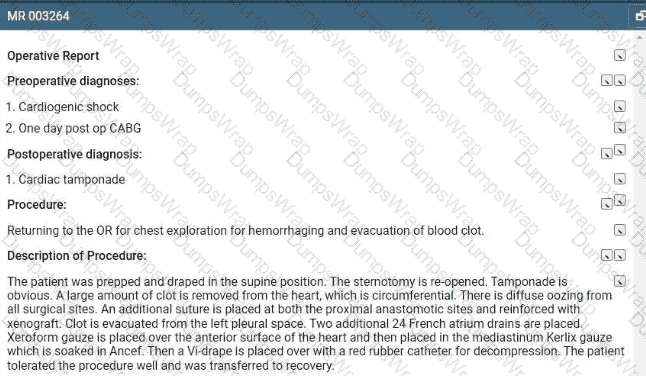
View MR 003264
What is the procedural coding?
A 44-year-old female patient came in for a planned laparoscopic total abdominal hysterectomy for endometriosis of the uterus. The surgeon attached the trocars, a scope is inserted examining
the uterus, abdominal wall, bilateral ovaries, and fallopian tubes. The surgeon decided to convert the laparoscopic procedure to an open total hysterectomy because of the extensive amount of
adhesions that need to be removed. A total hysterectomy was performed and due to removal of the extensive adhesions the surgery took longer than normal of 2 hours.
What CPT® and diagnosis codes are reported?
What is the medical term for a procedure that creates a connection between the gallbladder and the small intestine?
What is the medical term for a procedure that creates an opening between the bladder and the rectum?
An 8-year-old patient is placed under general anesthesia for treatment of a right orbital fracture due to a traumatic fall to the nose and face from a swing set. An on-call otolaryngologist is
asked to perform a general otolaryngologic examination to evaluate the patient. A mild nasal fracture is the diagnosis given by the otolaryngologist.
What is the CPT® and ICD-10-CM coding for the otolaryngologist ' s services?
A healthy 35-year-old undergoes EP study and ablation under general anesthesia.
What anesthesia coding is correct?
A 49-year-old patient arrives with hearing loss in his left ear. Impedance testing via tympanometry is performed.
What CPT® code is reported?
A 55-year-old patient was recently diagnosed with an enlarged goiter. It has been two years since her last visit to the endocrinologist. A new doctor in the exact same specialty group will be examining her. The physician performs a medically appropriate history and exam. The provider reviewed the TSH results and ultrasound. The provider orders a fine needle aspiration biopsy which is a minor procedure.
What E/M code is reported?
(A 42-year-old female is in the operative room to repair azone 2 flexor digitorum profundus (FDP) tendonlaceration involving her index finger with an associatedradial digital nerveinjury. The dorsal side of the FDP tendon was sutured. Next, themicroscopewas brought into place and the radial digital nerve was repaired using epineural sutures. What CPT® codes are reported?)
(Preoperative diagnoses:Bradycardia.
Postoperative diagnosis:Bradycardia.
Procedure performed:Dual-chamber pacemaker implantation.
Brief history:77-year-old female with recurrent syncope; evaluation revealed first-degree AV block, sinus bradycardia, bundle-branch block; bradyarrhythmia suspected; after discussion with her sister, dual-chamber pacemaker recommended; risks explained; consent obtained.
Procedure details:Taken to cardiac catheterization lab; positioned on cath table; prepped/draped standard; procedure challenging due to agitation despite adequate sedation; left infraclavicular area anesthetized with 0.5 cc Xylocaine; pacemaker pocket created; hemostasis with cautery; 9-French peel-away sheath used to introduce an atrial and a ventricular lead; leads positioned with excellent thresholds; secured with O-silk sutures over sleeves; pulse generator connected; pocket flushed with antibiotic solution; pacemaker/leads placed in pocket; incision closed in two layers; performed under fluoroscopic guidance.
Complication:None.
Plan:Return to recovery; discharge later this evening to nursing home with routine post-pacemaker care.
Question:What CPT® coding is reported for this procedure?)
A physician orders a CT scan of the abdomen without contrast.
What CPT® coding is reported?
A 7-year-old boy was brought 10 the ED by his mother after he had been playing with small beads and one got lodged in his right external ear canal. After examination, the physician decided to remove the foreign body from the external auditory canal using alligator forceps without anesthesia.
What CPT® code is reported?
A 5-year-old who has an allergy history experienced a possible reaction to peanuts. A quantitative, high-sensitive fluorescent enzyme immunoassay was used to measure specific IgE for recombinant peanut components. Results showed there was no reaction indicating the child has a peanut allergy.
What lab test is reported?
(An 8-day-old newborn, weighing 3 kilograms, is seen for a circumcision. A numbing cream is applied. A circumferential incision is made and the foreskin is excised with a scalpel. What CPT® coding is reported?)
A patient has a bone infection being treated with vancomycin. A therapeutic drug assay is performed to measure the concentration of vancomycin in the patient ' s blood.
What lab test is reported?
Refer to the supplemental information when answering this question:
View MR 874276
What E/M code is reported?
A patient is brought to the operating room with a right-sided peripheral vertigo. The provider makes a postauricular incision and uses an operating microscope to perform a mastoidectomy using a burr. He next destroys the semicircular canals, the utricle, and saccule completely removing the diseased labyrinth structures. The provider sutures the incision.
What CPT® code and ICD-10-CM codes are reported?
A patient has chronic cholesteatoma in the right middle ear. The otolaryngologist performed a tympanoplasty with a radical mastoidectomy, removing the middle ear cholesteatoma. Grafting technique was used to repair the eardrum without ossicular chain reconstruction.
What CPT® code is reported for this surgery?
A 1-year-old patient has bilateral supernumerary digits:
Left digit contains bone and joint → amputated
Right digit is a soft-tissue nubbin → simple excision
What CPT® coding is reported?
Ms. C is diagnosed with a supratentorial intracerebral hematoma, and the neurologist performs a craniectomy to access the hematoma. The hematoma is accessed, and a suction device is
used to remove it.
What CPT@ code is reported?
A 45-year-old female presents to the ED with chest pain. The provider has an Albumin Cobalt Binding Test to determine if the chest pain is ischemic in nature.
That lab test is reported?
(A 6-month-old child was brought to the hospital with severe breathing difficulties. After testing, the child was diagnosed withtracheal stenosis present from birth. The pediatric surgeon performed atracheoplasty(surgical widening of the trachea). What CPT® and ICD-10-CM codes are reported?)
(A 32-year-old visited a provider due to ongoing irritation and watering in his left eye. Suspecting an allergy, the provider carried out a test, introducing an allergenic extract into the mucous membrane inner lining of the eye. The patient’s eye is monitored for signs of an allergic reaction, such as redness and itching. What CPT® code is reported?)
A patient is sent to the hospital by his family care provider for admission due to a high fever and neck pain The patient is admitted to the hospital to rule out bacterial meningitis. The hospitalist admits the patient and orders a CBC. CMR Blood culture, CT of the head and chest, and a lumbar puncture (spinal tap). After review of the results, he determines the patient has bacterial meningitis and starts the patient on IV antibiotics.
What CPT® and ICD-10-CM codes are reported for the admission?
A 57-year-old woman with a physical status of 3 received general endotracheal anesthesia for a panniculectomy. The anesthesiologist personally performed the entire anesthesia service.
What CPT@ coding is reported for the anesthesia?
Refer to the supplemental information when answering this question:
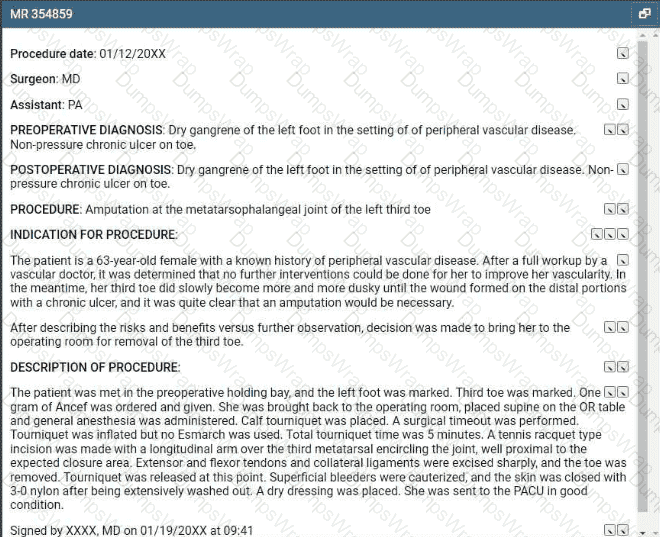
View MR 354859
What CPT® and ICD-10-CM coding is reported?
Which medical term refers to inflammation of the cornea?
